Glaucoma Treatment
An Introduction to the "Silent Thief of Vision"
Glaucoma is sometimes called the silent thief because it can slowly steal your sight before you realize anything's wrong. It's a leading cause of vision loss. The most common form of Glaucoma, primary open - angle Glaucoma, Develops Gradually, giving no warning signs. Many people aren't even aware they have an eye problem until their vision is extensively compromised.
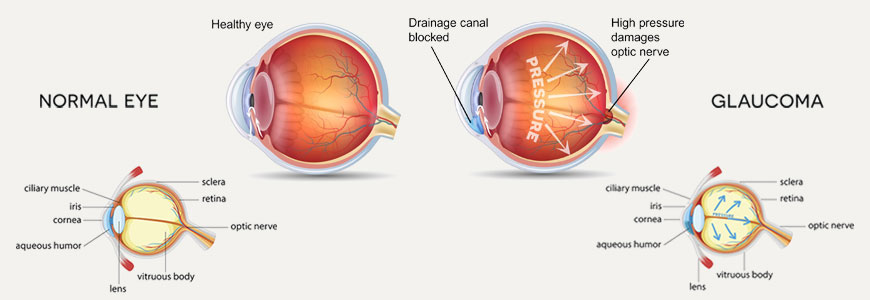
Glaucoma is not just one disease, but a group of them. The common feature of these diseases is damage to the optic nerve, usually accompanied by an abnormally high pressure inside your eyeball. The optic nerve is a bundle of more than a million nerve fibers at the back of your eye. It's like an electric cable made up of thousands of individual wires carrying the images from the inside back wall of your eyeball ( retina ) to your brain. Blind spots develop in your visual field when the optic nerve deteriorates, usually starting with your peripheral ( side ) vision. If left untreated, glaucoma may lead to blindness in both eyes.
Fortunately, medical advances have made it easier to diagnose and treat Glaucoma. If detected and treated early, glaucoma need not cause even moderate vision loss. But having Glaucoma does mean regular monitoring and treatment for the rest of your life.
Signs and Symptoms
Glaucoma occurs in several types, and signs and symptoms vary depending on the type of glaucoma you have. Primary open - angle glaucoma progresses with few or no symptoms until the condition reaches an advanced stage. As increased eye pressure continues to damage your optic nerve, you lose more and more of your peripheral vision. If Glaucoma is left untreated, you can develop tunnel vision and eventually lose all sight. Open - angle Glaucoma usually affects both eyes, although at first you may have vision loss in just one eye.
Acute angle - closure Glaucoma develops suddenly in response to a rapid rise in eye pressure. Permanent vision loss can occur within a day of the attack, so it requires immediate medical attention. An attack often happens in the evening or in a darkened room when the light is dim and your pupils have become relatively dilated. Pain may be severe.
Signs and symptoms include : Blurred vision, Halos around lights, Reddening of the eye, Severe eye pain, Nausea and vomiting.
Both open - angle and angle - closure Glaucoma can be primary or secondary conditions. They're called primary when the cause is unknown. They're called secondary when the condition can be traced to a known cause, such as an injury or an eye disease. Signs and symptoms of secondary glaucoma vary and depend on what's causing the Glaucoma.
Causes
Internal pressure in your eye, called intraocular pressure, allows your eye to hold its shape and function properly. Intraocular pressure is like air in a balloon - too much pressure inside the balloon affects its shape and may even cause it to pop. In the case of your eye, too much pressure can damage the optic nerve.
Fluids inside your eye help maintain the intraocular pressure. These fluids are the vitreous, which fills the vitreous cavity at the back of your eye, and the aqueous humor, which fills the anterior chamber at the front of your eye. Aqueous humor is continuously produced and circulated through the anterior chamber before draining out of your eye. This continuous flow of fluid nourishes the lens and the cornea and also removes unwanted debris. A healthy eye produces aqueous humor at the same rate that it drains fluid, thus maintaining a normal pressure.
Your eyes Drainage System
Aqueous humor exits your eye through a drainage system located at the angle formed where the iris and the cornea meet. Here it passes through a sieve - like system of spongy tissue called the trabecular meshwork and drains into a channel called Schlemm's canal. The fluid then merges into your bloodstream.
When the drainage system doesn't function properly - for example, if the trabecular meshwork becomes clogged - the aqueous humor can't filter out of the eye at its normal rate, and pressure builds within your eye. For reasons that doctors don't completely understand, increased eye pressure is often associated with gradual damage to the nerve fibers that make up the optic nerve.
Types of Glaucoma
Primary Open - Angle Glaucoma : This form, also called chronic open - angle Glaucoma, accounts for most cases of the disease. Although the drainage angle formed by the cornea and the iris remains open, the aqueous humor drains too slowly. This leads to fluid backup and a gradual buildup of pressure within your eye. Damage to the optic nerve is so slow and painless that a large portion of your vision can be lost before you're even aware of a problem.
The exact cause of primary open - angle Glaucoma remains unknown. It may be that the aqueous humor drains or is absorbed less efficiently with age, but not all older adults get this form of Glaucoma. About 2 percent of Americans older than age 40 have elevated eye pressure. For Americans older than 70, the number is 8 percent.
Angle - Closure : Angle - closure Glaucoma, also called closed - angle Glaucoma, is a less common form of the disease. This type of Glaucoma is a medical emergency that can cause vision loss within a day of its onset. It occurs when the drainage angle formed by the cornea and the iris closes or becomes blocked. Many people with this type of Glaucoma have a very narrow drainage angle, which may be an abnormality from birth. As you get older, your lens becomes larger, pushing your iris forward and narrowing the space between the iris and the cornea.
Whether the narrow drainage angle is an abnormality from birth or a result of aging, as this angle narrows, the iris gets closer to the trabecular meshwork. If it gets too close, the aqueous humor can't exit through the trabecular meshwork, resulting in a buildup of fluid and an increase in eye pressure. Angle - closure glaucoma can be chronic ( progressing gradually ) or acute ( appearing suddenly ). The acute form occurs when the iris is forced up against the trabecular meshwork and completely blocks the drainage of the aqueous humor.
Angle - closure Glaucoma is more common among farsighted people. Normal aging also may cause angle blockage. If you have a narrow drainage angle and your pupils become dilated, the angle may close and cause a sudden increase in eye pressure. This attack of acute angle - closure Glaucoma requires immediate treatment. Although an acute attack often affects only one eye, the other eye is at risk of an attack as well.
Several factors can cause your pupils to dilate, including darkness or dim light, stress or excitement, and certain medications. These medications include antihistamines, tricyclic antidepressants and eyedrops used to dilate your pupils. However, dilating eyedrops may not cause the angle to close until several hours after the drops are put in your eyes.
Secondary : Both open - angle and angle - closure glaucoma can be primary or secondary conditions. They're called primary when the cause of the condition is unknown. They're called secondary when the condition can be traced to a known cause, such as an injury or an eye disease. Secondary Glaucoma may be caused by a variety of Medical Conditions, Medications, Physical Injuries, and Eye Abnormalities or Deformities. Infrequently eye surgery can be associated with secondary Glaucoma.
Low - Tension : Low - tension Glaucoma is a poorly understood, though not uncommon, form of the disease. In this form, eye pressure remains within what is ordinarily thought to be the normal range, but the optic nerve is damaged nevertheless. Why this happens is unknown. Some experts believe that people with low - tension Glaucoma may have an abnormally sensitive optic nerve or a reduced blood supply to the optic nerve caused by a condition such as atherosclerosis, a hardening of the arteries caused by accumulation of fatty deposits ( plaques ) and other substances. Under these circumstances even normal pressure on the optic nerve seems to be enough to cause damage. Doctors don't completely understand the underlying causes of glaucoma. Although glaucoma is normally associated with increased eye pressure, people with normal or low eye pressure can experience vision loss. And people with higher than normal eye pressure may never experience optic nerve damage.
Risk Factors
If the internal pressure in your eye ( intraocular pressure ) is higher than what's considered normal, you're at increased risk of developing glaucoma, though not everyone with elevated intraocular pressure develops the disease. This makes it difficult to predict who will get Glaucoma.
Certain other factors increase your risk. Because chronic forms of glaucoma can destroy vision before any signs or symptoms are apparent, be aware of these factors :
Age : Age is a large risk factor in the development of Glaucoma. Everyone older than 60 is at increased risk of the disorder. For blacks however, the increase in risk becomes apparent earlier, after age 40.
Race : Blacks are significantly more likely to get Glaucoma than are whites, and they are much more likely to suffer permanent blindness as a result. Mexican - Americans also face an increased risk. Asian - Americans are at higher risk of angle - closure Glaucoma, and Japanese - Americans are more prone to low - tension Glaucoma. The reasons for these differences aren't clear.
Family History of Glaucoma : If you have a family history of Glaucoma, you have a much greater risk of developing Glaucoma. Glaucoma may have a genetic link, meaning there's a defect in one or more genes that may cause certain individuals to be more susceptible to the disease.
Medical Conditions : Diabetes increases your risk of developing Glaucoma. A history of high blood pressure or heart disease also can increase your risk, as can hypothyroidism. Routine use of coffee has recently been found to be associated with a slight increase in intraocular pressure.
Physical Injuries : Severe trauma, such as being hit in the eye, can result in increased eye pressure. Injury can also dislocate the lens, closing the drainage angle. Other risk factors include Retinal Detachment, eye tumors, and eye inflammations such as chronic uveitis and iritis. Certain types of eye surgery also may trigger secondary Glaucoma.
Nearsightedness : Being nearsighted, which generally means that objects in the distance look fuzzy without glasses or contacts, increases the risk of developing Glaucoma.
Prolonged Corticosteroid Use : Using corticosteroids for prolonged periods of time appears to put you at risk of getting secondary Glaucoma.
Eye Abnormalities : Structural abnormalities of the eye can lead to secondary Glaucoma. For example, pigmentary Glaucoma is a form of secondary glaucoma caused by pigment granules being released from the back of the iris. These granules can block the trabecular meshwork.
When to seek medical advice
Primary open-angle glaucoma gives few warning signs or symptoms until permanent damage has already occurred. That's why regular eye exams are the key to detecting glaucoma early enough for successful treatment. It's best to have routine eye checkups every two to four years after age 40 and every one to two years after age 65. Because African-Americans have a much higher risk of glaucoma, screening should begin every three to five years from age 20 to 29, and every two to four years after age 30.
Don't wait for problems of any kind to occur. If you have one or more risk factors for glaucoma, talk to your doctor about scheduling regular eye exams. Some tests can be performed by your regular doctor, but others need to be done by an eye-care specialist. In addition, be alert for signs or symptoms of an acute angle-closure glaucoma attack, such as a severe headache or pain in your eye or eyebrow, nausea, blurred vision, or rainbow halos around lights. If you experience any of these problems, seek immediate care at your local hospital emergency room. If you've received a diagnosis of glaucoma, establish a regular schedule of examinations with your doctor to be sure your treatment is helping maintain a safe pressure in your eyes.
Screening and Diagnosis
If your doctor suspects that you have Glaucoma, he or she may perform a series of tests to detect any signs of damage. Tests include :
Tonometry : Tonometry is a simple, painless procedure that measures your intraocular pressure. It is usually the initial screening test for Glaucoma.
Two common techniques are air - puff tonometry and applanation tonometry. Air - puff tonometry uses a puff of air to measure the amount of force needed to indent your cornea. An applanation tonometer is a sophisticated device that's usually fitted to a slit lamp. Slit lamps use an intense line of light - a slit - providing illumination of the cornea, iris, lens and anterior chamber, and allowing your doctor a good view of these structures. With tonometry, your doctor numbs your eyes with drops and has you sit behind the slit lamp, where a small flat - tipped cone pushes lightly against your eyeball. The force required to flatten ( applanate ) a small area of your cornea translates into a measure of your intraocular pressure.
Average normal eye pressures range from 10 to 21 or 22 millimetres of mercury ( mm Hg ), though most pressures are within 14 to 16 mm Hg. Doctors consider anyone with eye pressure greater than 22 mm Hg to be at risk of developing glaucoma and in need of careful monitoring for early signs of Glaucoma. Tonometry readings vary somewhat depending on a variety of factors including the thickness of your corneas and whether you've had laser surgery on your eyes. For these reasons, newer technologies are being investigated to improve the standard applanation instrument and obtain more accurate intraocular eye pressure measurements.
Test for Optic Nerve Damage : To check the fibers in your optic nerve, your eye doctor uses an instrument called an Ophthalmoscope or Biomicroscope, which enables him or her to look directly through the pupil to the back of your eye. Your doctor may also use laser light and computers to create a three - dimensional image of your optic nerve. This can reveal slight changes that may indicate the beginnings of Glaucoma. Your doctor may also make a detailed drawing of your optic nerves and take photographs of the optic nerves in order to monitor any changes that might occur at future visits.
Visual Field Test : To check how your visual field has been affected by Glaucoma, your doctor uses a perimetry test. One method, known as tangent screen perimetry, requires you to look at a screen with a target in the center. Your eye doctor or a technician manipulates a small object on a wand at different locations in your visual field. You indicate whenever you see the object come into view. By repeating this process over and over again, your entire visual field can be mapped.
Pachymetry : Your eyes are numbed for this test, which uses an ultrasonic - wave instrument to gauge the thickness of each cornea. The thickness of your corneas is an important factor for accurately diagnosing Glaucoma. If you have thick corneas, your eye pressure reading may seem high even though you don't have Glaucoma. Conversely, people with thin corneas can have low pressure readings, but have Glaucoma.
Other Tests : To distinguish between open - angle Glaucoma and angle - closure Glaucoma, your eye doctor may use a technique called gonioscopy, in which a special lens with an angled mirror is placed on your eye to inspect the drainage angle. Another test, tonography, can measure how fast fluid drains through the trabecular meshwork.
To Establish a Diagnosis of Glaucoma, Several Factors must be Present :
Elevated intraocular pressure, Areas of vision loss, Damage to your optic nerve, In Glaucoma, the optic disk shows visible signs of damage. The optic disk is the area where all of the nerve fibers come together at the back of your eye before exiting your eyeball. An optic disk that has been affected by Glaucoma appears indented, or excavated, as if someone scooped out part of the center of the disk. This condition is known as cupping. The normal contour and color of the disk may also be affected by the loss of nerve fibers.
Treatment
The treatment of Glaucoma is aimed at reducing intraocular pressure by improving aqueous outflow, reducing the production of aqueous or both. Doctors accomplish these treatment goals with eyedrops, systemic medications, laser treatment, surgery, or a combination of treatments.
If your doctor determines that you have elevated intraocular pressure, an excavated optic disk and loss of visual field, you'll likely be treated for Glaucoma. If you have only slightly elevated eye pressure, an undamaged optic nerve and no visual field loss, you may not need treatment, but your doctor may advise more frequent examinations to detect any future changes. If you have signs of optic nerve damage and visual field loss, even if your eye pressure is in the normal range, you may need treatment to lower eye pressure further, which may help slow the progression of Glaucoma.
Glaucoma can't be cured, and damage caused by the disease can't be reversed. But with treatment, Glaucoma can be controlled. Eye drops, oral medications and surgical procedures can prevent or slow further damage.
Lifelong Treatment
Having Glaucoma means you'll need to continue treatment for the rest of your life. Because the disease can progress or change without your being aware of it, your treatment may need to be adjusted over time. Regular check - ups and adherence to a treatment plan may seem burdensome, but they're essential to prevent vision loss.
Keeping your eye pressure under control can prevent further damage to the optic nerve and continued loss of your visual field. Your eye doctor may focus on lowering your intraocular pressure to a level that's unlikely to cause further optic nerve damage. This level is often referred to as the target pressure and will probably be a range rather than a single number. Target pressure differs for each person, depending on the extent of the damage and other factors. Your target pressure may change over the course of your lifetime.
Topical eye medications are the most common early treatment for Glaucoma. Reducing the pressure in the eyes has been shown to reduce the progression of visual field loss. Standard practice has been to move on to surgery if medications are ineffective or if the Glaucoma patient has difficulty in adhering to the medical therapy recommendations. However, surgery is also a relatively safe and effective initial treatment.
Eye drops
Glaucoma treatment often starts with medicated eyedrops. Doctors prescribe several types of drops. Be sure to use the drops exactly as prescribed to control your intraocular pressure . Skipping even a few doses can cause damage to the optic nerve to worsen. Some drops need to be applied several times each day, and others must be used just once a day. Inform your doctor of all other medications you're taking, to avoid any undesirable drug interactions.
Because some of the eyedrops are absorbed into your bloodstream, you may experience side effects unrelated to your eyes. To minimize this absorption, close your eyes for one to two minutes after putting the drops in. Press lightly at the corner of your eye near your nose to close the tear duct, and wipe off any unused drops from your eyelid. Your doctor may prescribe more than one type of eyedrop. If you're using more than one, ask your doctor how long to wait between applications.
The types of Eyedrops that Doctors most Commonly Prescribe Include :
Beta - Blockers : These reduce the production of aqueous humor. Examples include levobunolol timolol, carteolol, betaxolol and metipranolol. Possible side effects include Difficulty Breathing, Slowed Pulse, Hair Loss, Lower Blood Pressure, Impotence, Fatigue, Weakness, Depression and Memory Loss. If you have asthma, bronchitis or emphysema or if you have diabetes and use insulin, medications other than beta - blockers may be recommended because beta - blockers may worsen breathing problems.
Alpha - Adrenergic Agents : These reduce the production of aqueous humor. Examples include Apraclonidine and Brimonidine. Possible side effects include Fatigue, Dizziness, Red, Itchy or Swollen Eyes, Dry Mouth and Allergic Reactions.
Carbonic Anhydrase Inhibitors : These medications, which include Dorzolamide and Brinzolamide, reducethe amount of aqueous humor. Possible side effects include frequent urination and a tingling sensation in the fingers and toes, but these occur more frequently when a carbonic anhydrase inhibitor is taken orally. If you have an allergy or sensitivity to sulpha drugs, don't use these medications unless there's no alternative.
Prostaglandin Analogues : These eyedrops increase theoutflow of aqueous humor. These hormone - like substances, which include latanoprost, bimatoprost and travoprost, may be used in conjunction with a drug that reduces production of aqueous humor. There has been a trend away from using these agents as a first line therapy for glaucoma. Possible side effects include mild reddening and stinging of the eyes and darkening of the iris, changes in the pigment of the eyelid skin, and blurred vision from swelling of the retina.
Miotics : Miotics, such as pilocarpine, increase the outflow of aqueous humor. Possible side effects include Pain Around or Inside the Eyes, Brow Ache, Blurred or Dim Vision, Near - Sightedness, Allergic Reactions, a Stuffy Nose, Sweating, Increased Salivation, and Occasional Digestive Problems.
Epinephrine Compounds : These also increasethe outflow of aqueous humor. Possible side effects include Red Eyes, Allergic Reactions, Palpitations, an Increase in Blood Pressure, Headache and Anxiety.
Oral Medications
If eyedrops alone don't bring your eye pressure down to the desired level, your doctor may also prescribe an oral medication. Doctors commonly prescribe carbonic anhydrase inhibitors, such as acetazolamide and methazolamide, for Glaucoma. Take these pills with meals to reduce side effects. You can help to minimize the potassium loss that these medications can cause by adding bananas and apple juice to your diet.
When you first start taking these oral medications, you may experience a frequent need to urinate and a tingling sensation in your fingers and toes. After several days, these symptoms usually disappear. Other possible side effects of carbonic anhydrase inhibitors include Rashes, Depression, Fatigue, Kidney Stones, Lethargy, Stomach Upset, a Metallic Taste in Carbonated Beverages, Impotence and Weight Loss.
Neuroprotective Drugs
Lowering the intraocular pressure provides only a partial solution when it comes to preserving vision in people with Glaucoma. Several clinical trials are under way to learn if certain drugs may help protect the optic nerve from damage associated with Glaucoma. Some are investigating the potential neuroprotective effects of brimonidine, a topical eye medication that may already be prescribed for Glaucoma. Another is investigating the potential neuroprotective effect of memantine, an oral medication generally used in the treatment of Alzheimer's disease.
Surgery
You may Need Surgery to Treat Glaucoma if you can't Tolerate Medications or if they're Ineffective. Doctors use Several Types of Surgery to Treat Glaucoma :
Laser Surgery : In the last couple of decades, a procedure called trabeculoplasty has been used increasingly in the treatment of open - angle Glaucoma. The doctor uses a high - energy laser beam to shrink part of the trabecular meshwork, which causes other parts of the meshwork to stretch and open up. This helps aqueous humor drain more easily from the eye.
This type of laser surgery is an office procedure that takes 10 to 20 minutes. You'll be given an anesthetic eyedrop, seated at a slit lamp and fitted with a special lens on your eye. The doctor aims the laser through the lens at the trabecular meshwork and applies burns to it. You will see bright flashes of light. Usually, you can immediately resume normal activities without discomfort. The doctor will usually check your eye pressure one to two hours after the procedure and several times in the following weeks. It may take a few weeks before the full effect of the surgery becomes apparent. In almost all cases, laser surgery for Glaucoma initially lowers intraocular pressure. After time, however, intraocular pressure may begin to increase.
Conventional Surgery : If eyedrops and laser surgery aren't effective in controlling your eye pressure, you may need an operation called a filtering procedure, usually in the form of a trabeculectomy. This procedure is done in a hospital or an outpatient surgery center. You'll receive medication to help you relax and eyedrops and usually an injection of anesthetic to numb your eye. Using delicate instruments under an operating microscope, your surgeon creates an opening in the sclera - the white of your eye - and removes a small piece of the trabecular meshwork.
The aqueous humor can now freely leave the eye through this hole. As a result your eye pressure will be lowered. The hole is covered by the conjunctiva, so there's not an open hole in your eye. This procedure works best if you haven't had any previous eye surgery. Your doctor will check your eye during several follow - up visits. You'll need to use antibiotic and anti - inflammatory eyedrops for some time after the operation to fight infection and scarring of the newly created drainage opening. Scarring is a particular problem for young adults, blacks and people who have had cataract surgery. Although Glaucoma surgery may preserve current vision, it can't restore already lost vision. Sometimes a single surgical procedure may not lower eye pressure enough, in which case you'll need to continue using Glaucoma drops or have another trabeculectomy operation.
Drainage implants. Another type of operation, called drainage implant surgery, may be an option for people with secondary Glaucoma or for children with glaucoma. Like the trabeculectomy, drainage implant surgery is performed at a hospital or an outpatient clinic. You'll receive medication to help you relax and eyedrops and an anesthetic to numb your eye. Then the doctor inserts a small silicone tube in your eye to help drain aqueous humor. After the surgery you'll wear an eye patch for 24 hours and use eyedrops for several weeks to fight infection and scarring. Your doctor will check your eyes several times in the weeks that follow. Possible complications from Glaucoma surgery may include infection, bleeding, eye pressure that remains too high or too low, and, potentially, loss of vision. Having eye surgery may also speed up the development of cataracts. Most of these complications can be effectively treated.
Treating Acute Angle - Closure Glaucoma
Acute angle - closure Glaucoma is a medical emergency. When you come in with this condition, doctors may administer several medications to reduce eye pressure as quickly as possible. You'll also likely have a laser procedure called iridotomy.
In this procedure, a laser beam creates a small hole in your iris to allow aqueous humor to flow more freely into the anterior chamber where it then has normal access to the trabecular meshwork. Once aqueous humor can reach the trabecular meshwork again, the fluid can drain as it normally does. Many doctors recommend an iridotomy on the other eye at a later date because of the high risk that it too will have an attack within the next few years.
Prevention
Until recently, there was no proven way to prevent Glaucoma. But a large multicenter trial, supported by the National Eye Institute, found that when glaucoma eyedrops were given daily to people with elevated eye pressure ( above 24 mm Hg ), they reduced eye pressure an average of 22 per cent. More important, the researchers discovered that daily use of eyedrops can reduce the risk of developing Glaucoma by nearly half in blacks with elevated eye pressure.
Another study found that cholesterol lowering medications reduced the risk of open - angle Glaucoma, especially for people who already have cardiovascular disease. Although this may be an added benefit for those already taking these medications to reduce their cholesterol levels, more studies need to be done to confirm the reduction in risk of Glaucoma.
Frequent Monitoring
Regular checkups can help detect the disease in its early stages before irreversible damage has occurred. As a general rule, have eye exams every two to four years if you're between the ages of 40 and 65 and every one to two years if you're older than 65.
Your doctor will likely recommend more frequent monitoring if you're at increased risk of developing Glaucoma. For example, a family history of glaucoma puts you at increased risk of developing Glaucoma and is a reason for more frequent monitoring. You may also need even more frequent checkups if you have received a diagnosis of abnormally high intraocular pressure or have a history of serious eye injury.
Self - Care
The most important thing you can do if you have Glaucoma is take your medications exactly as prescribed. Frequent eye exams will help your doctor monitor your eye pressure and keep you and your doctor aware of any changes in your vision.
Other Self - Care Tips :
Maintain a Healthy Diet : Eat a healthy diet full of fruits and vegetables to ensure that you get enough vitamins and minerals. Some that are especially important to your eye health include Vitamin A, Vitamin C, Vitamin E, Zinc and Copper. Drink fluids in small amounts over the course of a day. Drinking a quart or more of any liquid within a short time may increase eye pressure. Limiting caffeine to low or moderate levels may be helpful.
Exercise Regularly : People with open - angle Glaucoma who exercise regularly - at least three times a week may be able to moderately reduce their eye pressure. However, angle - closure glaucoma isn't affected by exercise, and people with pigmentary Glaucoma, a form of secondary Glaucoma, may experience increased eye pressure after exercise. Also, yoga and other exercises that put you in a head - down position may increase the pressure in your eyes. Talk to your doctor about an appropriate exercise program.
Don't Depend on Herbal Remedies for the Primary Care of Glaucoma : A number of herbal supplements, such as bilberry, are advertised as Glaucoma remedies. Bilberry has not been proved effective in preventing or treating Glaucoma and should never be used in place of proven therapies. Always be cautious about herbal supplements and discuss them with your doctor before trying them.
Find Healthy ways to Cope with Stress : Stress may trigger an attack of acute angle - closure Glaucoma. Relaxation techniques may be helpful in dealing with stress.
Wear Proper Eye Protection : Eye trauma can result in increased eye pressure. Wear safety glasses or goggles when you play sports, use tools or machinery, or work with chemicals.